















Claim 1: Autism in the United States has risen significantly in recent decades.
Analysis:
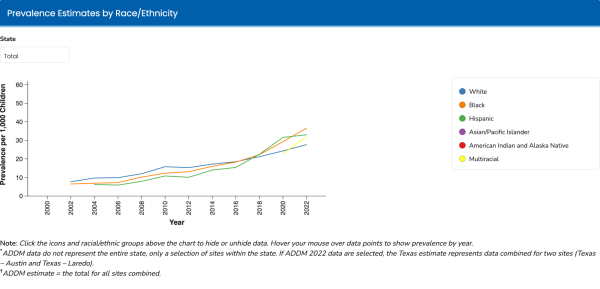
Trump framed his argument around prevalence, saying that “just a few decades ago, one in 20,000 children had autism, then one in 10,000 … now it’s 1 in 31. For boys, it’s 1 in 12,” and at points citing figures as low as 1 in 10.
Recent federal estimates partially align with the first part of that claim, but not the most extreme figures. The Centers for Disease Control and Prevention’s Autism and Developmental Disabilities Monitoring Network most recently reported an estimated prevalence of about 1 in 31 children. For boys, the estimate was 49.2 per 1,000 – roughly 1 in 20 – about half as common as Trump stated.
Public health officials caution that rising diagnoses do not necessarily mean more children have autism spectrum disorder. The CDC says the upward trend has largely been interpreted as improved and more equitable identification, particularly among groups that previously faced barriers to diagnostic evaluations and services.
Verdict:
His quantitative statements are largely supported by reputable statistics, but the primary understanding of prevalence versus awareness differs from the current scientific consensus.
Claim 2: More primitive societies that don’t use modern medicine have lower rates of autism.
Analysis:
“There are certain groups of people that don’t take vaccines and don’t take any pills who have no autism. Does that tell you something?” Trump asks, later mentioning Cuba and the Old Order Amish as examples.
This conflates correlation and causation; the idea that vaccination rates are proportional to screened autism often reflects that limited access to medical care coincides with less robust screening and diagnostic procedures.
Autism research has been conducted on these more secluded populations, with multiple studies finding existing autism in the Amish. The recorded rate – roughly 1 in 271 – is significantly lower than the latest national findings; however, this disparity can likely be attributed to more modern diagnostic tools and observed genetic differences.
Verdict: Autism rates in this population – when diagnosed with modern tools – are still higher than historical averages, making it unlikely that vaccines are to blame.
Claim 3: Tylenol during pregnancy increases autism risk.
Analysis:
President Trump ordered “the FDA [to notify] physicians that the use of acetaminophen, which is commonly known as Tylenol, during pregnancy can be associated with a very increased risk of autism,” saying that there are a “small number of cases” in which Tylenol should be used for pain relief or fever reduction.
The latest research on this is still unclear. Some studies have found a possible link between acetaminophen use in pregnancy and autism, but experts in the field, such as Dr. Zeyan Liew, associate professor of epidemiology at Yale, consider the data to be “constantly evolving.” Liew discourages vilifying treatment options until more research is available, recommending case-by-case consultation above anything else.
Verdict: While further investigation is needed, Tylenol remains the commonly recommended over-the-counter pain reliever in pregnancy, and any dosage decisions should be discussed with a physician.
Claim 4: Spacing out vaccinations in babies reduces side effects.
Analysis:
At the event, Trump said the “vat of 80 different vaccines” doctors “pump” into a “little fragile child” would be better spread “over a period of four times or five times” across several years. U.S. pediatric schedules do not give dozens of shots at once; combination vaccines reduce needle sticks, and a child may get several shots per visit to protect against many diseases, not “80 vaccines” at a time.
The CDC has established immunization schedules, accounting for research-based variances in effectiveness for children. One observable exception is the measles-mumps-rubella-varicella combo, which could have short-term effects, but most clinicians account for this during administration.
These schedules are frequently updated with the latest information, ensuring consistent and relevant administration practices.
Verdict: False. America’s healthcare system already accounts for these imbalances and orients itself to maximize accessibility to immunizations, with any exceptions in mind.